Statins: The Conversation Your GP Didn’t Have Time For

At some point in your 50s, there’s a reasonable chance a GP will look at your cholesterol numbers and suggest a statin. The appointment will be running late. You’ll have approximately ninety seconds to process what is being proposed before the next patient is waiting. You’ll leave with either a prescription or a vague sense that you probably should have asked more questions — and no clear idea which.
Statins are the most prescribed medication in the UK. Around eight million people take them daily. They are, in certain situations, genuinely life-saving drugs with decades of robust evidence behind them. However, they are also prescribed in situations where the evidence is considerably murkier, the benefits more modest, and the lifestyle alternatives more effective than most people are told.
This is the conversation your GP didn’t have time for.
⚡ What You’ll Learn in the Next 5 Minutes
- What statins actually do — and what cholesterol really means for your health
- Who the evidence clearly supports taking them — and who it doesn’t
- The side effects that are real, the ones that are overstated, and how to tell the difference
- The lifestyle interventions that genuinely compete with statins for lower-risk patients
- The exact questions worth asking your GP before you decide
First — What Statins Actually Do
Statins work by inhibiting an enzyme in the liver called HMG-CoA reductase, which is involved in producing cholesterol. Less enzyme activity means less cholesterol produced — specifically LDL cholesterol, the type most associated with cardiovascular risk. However, statins also have anti-inflammatory effects that are independent of their cholesterol-lowering action, which is one reason they work better than simply reducing cholesterol through diet alone in some patients.
It’s worth pausing on the cholesterol question itself, because the picture is more nuanced than “high cholesterol is bad.” LDL cholesterol is not a single thing — it comes in different particle sizes, and small dense LDL particles are considerably more dangerous than large buoyant ones. Total cholesterol on its own is a relatively poor predictor of cardiovascular risk. What matters more is the ratio of LDL to HDL, the presence of other risk factors, and increasingly, markers like apolipoprotein B and Lp(a) that your standard NHS panel probably doesn’t measure.
This context matters because the decision about whether to take a statin should not be based on a single cholesterol number in isolation. It should be based on your overall cardiovascular risk profile — which includes age, sex, blood pressure, smoking status, diabetes, family history, and yes, cholesterol. That composite risk is what the QRISK score your GP uses is designed to capture. Understanding what’s actually driving your risk is the foundation of a sensible decision, and it connects directly to the broader work of slowing biological ageing naturally after 50 — cardiovascular health sits at the centre of that picture.
Who the Evidence Clearly Supports
There are two broad categories of statin use, and the evidence looks very different for each.
Secondary prevention means using statins in people who have already had a heart attack, stroke, or been diagnosed with cardiovascular disease. Here the evidence is overwhelming and largely uncontested. Statins in this group reduce the risk of a further cardiovascular event significantly — the absolute risk reduction is meaningful, the benefit clearly outweighs the risk, and the recommendation to take them is about as solid as medical guidance gets.
Primary prevention means using statins in people who have not yet had a cardiovascular event but are considered at elevated risk. This is where the picture gets considerably more complicated — and where the conversation your GP didn’t have time for becomes most important.
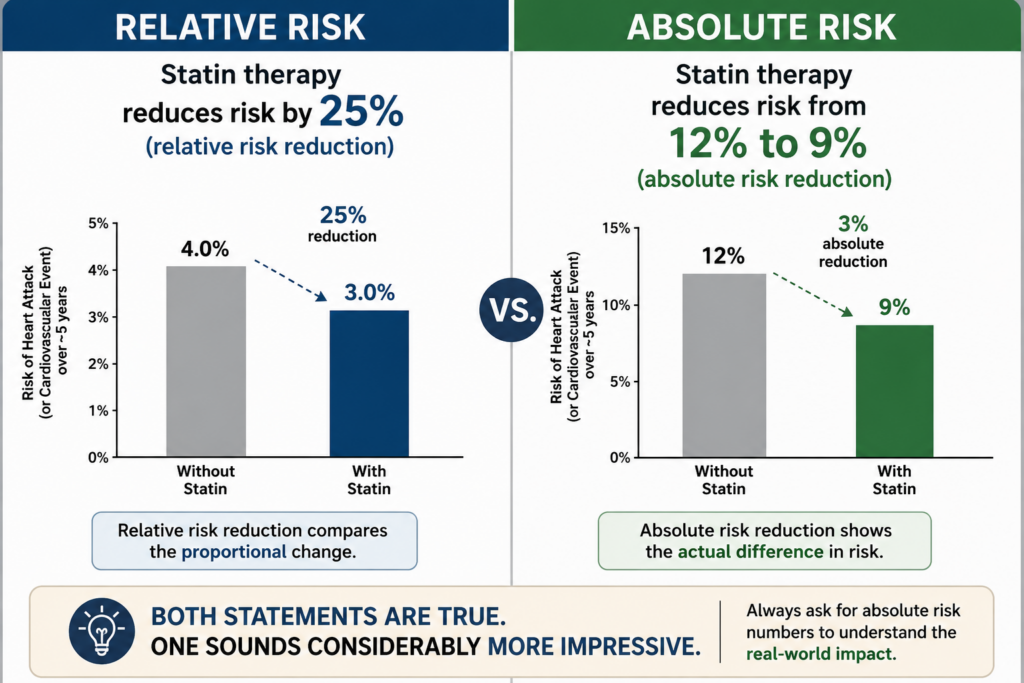
For primary prevention, the NHS currently recommends offering statins to people with a QRISK score of 10% or above — meaning a 10% or greater chance of having a cardiovascular event in the next ten years. However, the absolute benefit for someone at, say, 12% risk is quite different from the benefit for someone at 30% risk, even though both might receive the same prescription. A statin that reduces your relative risk by 25% sounds compelling. That same statin reducing your absolute risk from 12% to 9% over ten years — a 3 percentage point reduction — sounds rather different, and is a more honest representation of what the data shows for lower-risk primary prevention patients.
None of this means statins are wrong for primary prevention patients. It means the decision deserves a proper conversation — one that includes your actual QRISK score, what’s driving it, what the realistic absolute benefit is, and what the alternatives look like.
Side Effects — What’s Real and What’s Overstated
Statin side effects have become a significant online topic, which has led to two problems simultaneously: some people experiencing real side effects being dismissed, and some people stopping statins they genuinely need based on misinformation. Both happen, and both have consequences.
Muscle pain (myalgia) is the most commonly reported side effect and it is real. Studies suggest somewhere between 5–10% of statin users experience muscle aches, though the range in the literature is wide. In rare cases, statins can cause a more serious condition called rhabdomyolysis — a breakdown of muscle tissue that can damage the kidneys. This is uncommon but worth knowing about, particularly if you experience severe muscle pain or notice dark urine.
Elevated liver enzymes occur in a small percentage of users. Routine liver function monitoring is sometimes recommended when starting statins, though guidelines have moved away from routine ongoing monitoring for people tolerating them well.
Increased blood sugar is a less-discussed but real effect of statins. Research has shown that statins modestly increase the risk of developing type 2 diabetes — by approximately 10–12% in relative terms. For most people already at cardiovascular risk, the cardiovascular benefit outweighs this. However, for people on the borderline of pre-diabetes, it is a relevant consideration and worth discussing with your GP. The connection between inflammation, blood sugar regulation, and cardiovascular risk is something we explore further in our piece on how to reduce inflammation naturally.
Cognitive effects — memory problems and “brain fog” — are frequently cited online but the evidence here is weak. Large studies have not found a consistent cognitive effect from statins, and some research suggests statins may actually be protective against dementia. This is an area where anecdote has significantly outrun evidence.
The most important point on side effects: if you experience symptoms you think may be related to your statin, tell your GP rather than simply stopping. Different statins have different side effect profiles, different doses behave differently, and switching from one statin to another resolves the problem for many people who couldn’t tolerate the first.
The Lifestyle Alternatives — Taken Seriously, Not Dismissed
For people in the lower ranges of primary prevention — QRISK scores between 10–20%, no previous cardiovascular events, no diabetes — lifestyle intervention can produce cholesterol and cardiovascular risk reductions that genuinely compete with statin therapy. This is not alternative medicine. This is mainstream cardiology, and it tends to get undersold in short appointments.
Diet is the most powerful lever. Replacing saturated fats with unsaturated fats, increasing soluble fibre (oats, legumes, fruit, vegetables), and reducing processed food can lower LDL cholesterol by 20–30% in motivated patients — comparable to a low-dose statin. The portfolio diet, developed specifically to maximise cholesterol-lowering through food, has produced LDL reductions of around 30% in clinical trials. How you distribute protein and manage overall dietary quality matters here — our article on the role of protein in ageing covers the dietary framework in more detail.
Exercise — specifically aerobic exercise — raises HDL cholesterol and reduces triglycerides, improving the overall cardiovascular risk profile even without dramatic LDL changes. Resistance training adds further metabolic benefit through improved insulin sensitivity.
Weight management — even modest reductions in visceral fat (the fat around the organs, not simply subcutaneous fat) produce meaningful improvements in lipid profiles and blood pressure.
Alcohol reduction is one of the most underappreciated interventions. Alcohol raises triglycerides, increases blood pressure, and contributes to weight gain — three of the key cardiovascular risk factors. Reducing intake has rapid and measurable effects on the lipid profile.
Time-restricted eating — the most evidence-backed form of intermittent fasting — has shown modest but real benefits for lipid profiles and metabolic health in several studies. Our piece on whether intermittent fasting is good for ageing covers the current evidence carefully.
Sleep quality is also worth mentioning here — and it tends to be ignored entirely in cardiovascular consultations. Chronic poor sleep raises cortisol, drives inflammation, worsens insulin resistance, and increases blood pressure. As we explore in our piece on the importance of sleep for longevity, fixing sleep is one of the highest-leverage things you can do for cardiovascular health — and it costs nothing.
| Intervention | LDL Effect | Wider Cardiovascular Benefit | Evidence Quality |
|---|---|---|---|
| Statin (standard dose) | 30–50% reduction | Anti-inflammatory, plaque stabilisation | ✅ Very strong |
| Dietary intervention (portfolio diet) | 20–30% reduction | Blood pressure, weight, inflammation | ✅ Strong |
| Aerobic exercise | Modest LDL reduction, raises HDL | Blood pressure, insulin sensitivity, weight | ✅ Strong |
| Weight loss (5–10% body weight) | 10–20% reduction | Blood pressure, triglycerides, blood sugar | ✅ Strong |
| Alcohol reduction | Reduces triglycerides notably | Blood pressure, weight, liver health | ✅ Good |
| Sleep improvement | Indirect — via inflammation and cortisol | Blood pressure, insulin resistance, inflammation | ✅ Good |
The Questions Worth Asking Your GP
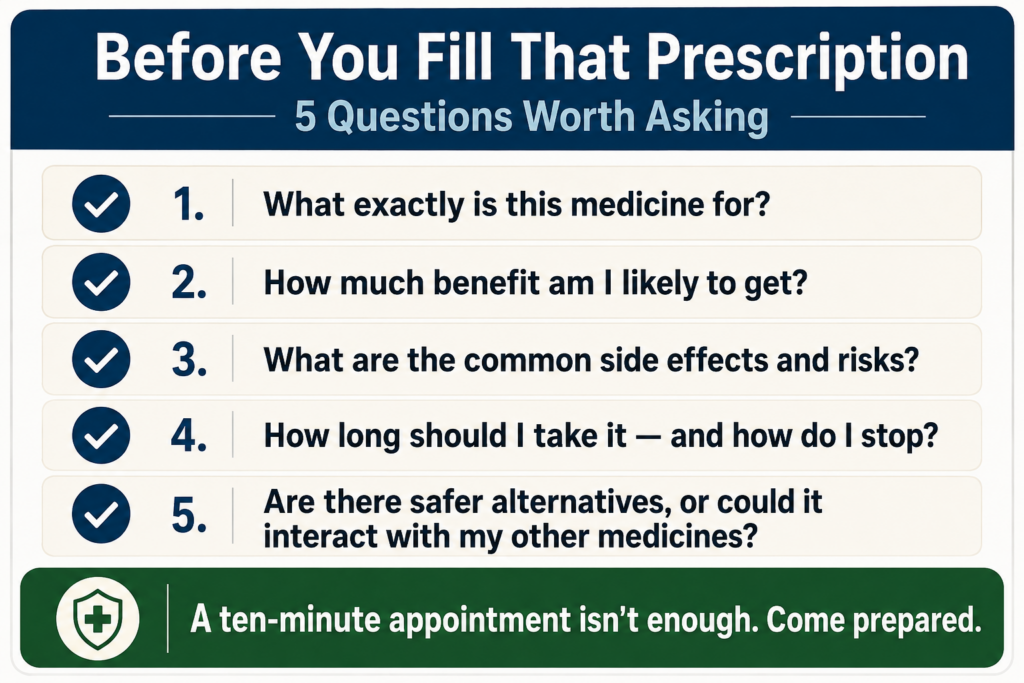
If you’re facing a statin decision — whether for the first time or as a review of an existing prescription — these are the questions that will get you the most useful information:
- “What is my actual QRISK score — and what’s driving it?” Understanding whether your risk is primarily driven by blood pressure, family history, cholesterol, or lifestyle factors matters enormously for knowing what to address.
- “What is my absolute risk reduction if I take a statin — not just the relative risk reduction?” Ask for the actual numbers. A 25% relative risk reduction means something very different at 30% baseline risk versus 10%.
- “If I commit to serious lifestyle changes for three months, can we retest before deciding?” For lower-risk primary prevention patients, this is a completely reasonable request. Not all GPs will agree, but many will.
- “If I experience side effects, what are my options?” There are multiple statins at multiple doses. Knowing there are alternatives before you start reduces the chance of abandoning treatment unnecessarily.
- “Should we also be looking at my Lp(a) and apolipoprotein B levels?” These markers give a more complete picture of cardiovascular risk than standard cholesterol panels and are increasingly available on the NHS.
If you haven’t had a recent NHS Health Check or comprehensive blood panel, that is the logical starting point before any statin conversation. Our guide to the health checks worth asking for after 50 covers exactly what to request and how to request it.
FAQ — Things People Actually Ask
Can I stop taking statins if I change my lifestyle significantly?
Possibly — but never without discussing it with your GP first and certainly not if you’re on statins for secondary prevention following a cardiovascular event. For primary prevention patients who have made sustained, significant lifestyle changes, it is a reasonable conversation to have. Some GPs will agree to a supervised trial period off statins with monitoring. What you should never do is simply stop without medical guidance and without a plan to monitor your risk.
Are newer cholesterol medications better than statins?
PCSK9 inhibitors are a newer class of cholesterol-lowering drugs with impressive LDL-reducing effects — considerably more powerful than statins in some cases. However, they are currently reserved for people with familial hypercholesterolaemia or those who cannot tolerate statins, primarily due to cost. They are not a routine alternative for most people currently being offered statins.
My cholesterol has always been high — should I be more worried?
Not necessarily. Familial hypercholesterolaemia — genetically elevated cholesterol — is a specific condition that does warrant more aggressive treatment. However, chronically elevated cholesterol without other risk factors in an otherwise healthy person represents a different risk picture from someone with elevated cholesterol plus high blood pressure, pre-diabetes, and a smoking history. Your QRISK score incorporates all of these factors together, which is why a single cholesterol number in isolation tells you relatively little.
What’s the single most important thing I can do this week?
If you’re currently taking a statin and have never had a proper conversation about your QRISK score and what’s driving it — book a medication review with your GP and ask for that conversation. If you’ve been told your cholesterol is high but haven’t been offered a statin yet, ask for your QRISK score and use it as the basis for a real discussion about your options. Knowledge first, decision second.
One Thing to Do This Week
Ask your GP — at your next appointment or in a telephone review — for your current QRISK score. Write it down. Then ask what the single biggest driver of that score is. That answer will tell you more about where to focus your energy than any supplement, screening, or prescription decision. It takes two minutes and changes the entire conversation.
Want to Go Deeper?
If this has prompted you to think more seriously about your cardiovascular health — and the lifestyle factors that influence it more than most people realise — we’ve put together guides covering the evidence-based interventions that actually move the needle.
Browse the full guides library at Slowing the Clock →
Take what’s useful. Leave what isn’t. That’s always the idea.